





The Background on Factor VIII
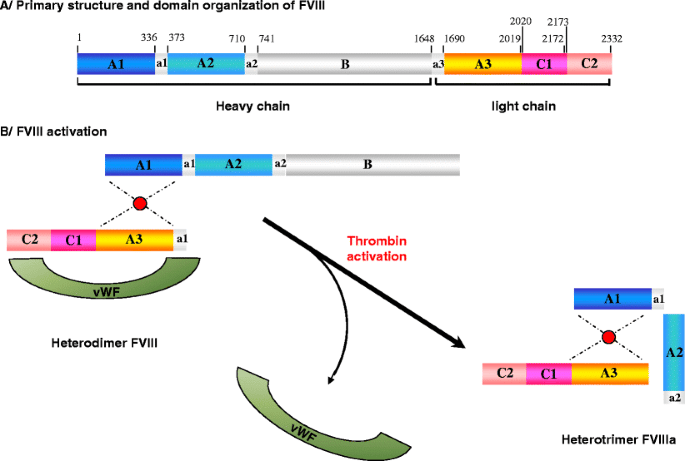
Factor VIII plays an essential role in blood clotting since defects in this gene result in hemophilia A and why it is also known as an anti-hemophilic factor (AHF). Factor VIII is produced in the liver sinusoidal cells and endothelial cells outside the liver, from where it travels throughout the entire body. Factor VIII protein consists of six domains: A1-A2-B-A3-C1-C2, and is homologous to factor V. Activation of factor VIII to factor VIIIa is done by cleavage and release of the B domain. This results in the protein being divided into heterodimeric structures made of heavy chains belonging to the A1 and A2 domains and another light chain belonging to the A3, C1, and C2 domains.
Factor VIII remains inactive while in the plasma and circulating all around the body. In this condition, it is tightly bound to the von Willebrand factor until an injury that damages blood vessels occur. In response to injury, coagulation factor VIII is activated and separates from the von Willebrand factor. The active protein (sometimes written as coagulation factor VIIIa) interacts with another coagulation factor called factor IX. This interaction sets off a chain of additional chemical reactions that form a blood clot.[8]
Factor VIII is no doubt an important molecule, which if the body lacks functional copies will undeniably cause the disorder called hemophilia A. Without this one molecule’s presence will result in excessive bleeding in case of a minor injury or slightest damage tissue.
Intravenous prophylactic clotting factor replacement therapy is commonly used to treat hemophilia A. However, it is not without limitations because there are infections, clots forming at the tip of the catheter, and some patients’ immune systems develop antibodies against these foreign bodies which makes the treatment ineffective over time.
However, a lot of doubts remain about the quantitation and activity of anti-factor VIII antibodies in hemophilia patients. This article will address these questions and a few other frequently asked ones.
- Q) How to Determine the Quantitation of Anti-Factor VIII Antibodies?
Antibodies in hemophilia A patients can undermine the therapeutic qualities of recombinant or plasma concentrate factor VIII administration. Studies largely focused on the presence of inhibitory antibodies ignoring the quantitation of noninhibitory anti-FVIII antibodies in human plasma. To carry out the investigation, an affinity-purified human antibody isolated from hemophilia patients was used as a calibrator. The experiment aimed to compare the difference in binding between human plasma samples and the calibrator on recombinant FVIII (rFVIII). Plasma samples were collected from 150 healthy donors and 39 inhibitor-negative hemophilia A subjects. These samples were run with 4 inhibitor-positive hemophilia A plasma samples as controls. Following here are the results:
- The four individuals used as controls had a detectable anti-FVIII antibody.
- Thirteen inhibitor negative subjects came out positive for the anti-FVIII antibody.
This method may be useful to treat a hemophilia A patient with a factor VIII inhibitor by informing medical staff to employ substitutes for rFVIII with these patients.
- Q) How to Measure Factor VIII Activity?
To get an idea of factor VIII activity, an activated partial thromboplastin time (aPTT) is used. A mixture of the diluted patient sample and factor VIII-deficient plasma is made. The mixture starts clotting after some time. This time is measured. The clotting time is then compared with the clotting time a normal plasma would take.
- Q) How Do the Extended Half-Life replacement therapies affect the aPPT-based factor VIII activity and inhibitor assay?
The PPT reagent used by the laboratory plays an important role in how the extended half-life replacement therapies will affect the activity levels. The difference in the effect is mainly due to the type of activator that might be present in the reagent.
- Q) What Might Happen If the Factor VIII Activity Gets Too High?
Factor VIII is a positive acute-phase reactant. In case a person is under a lot of stress or is facing inflammatory conditions or performs too much exercise, his or her factor VIII levels might shoot up. Higher levels increase the risk of venous thrombosis. Treatment for this condition would be the administration of anti-factor VIII antibodies.
Contact Green Mountain antibodies for a full range of services for creating new monoclonal antibodies or producing antibodies: 802-865-6230